Research
My research develops novel statistical methodology with applications in health sciences
Causal Inference for Complex Treatments
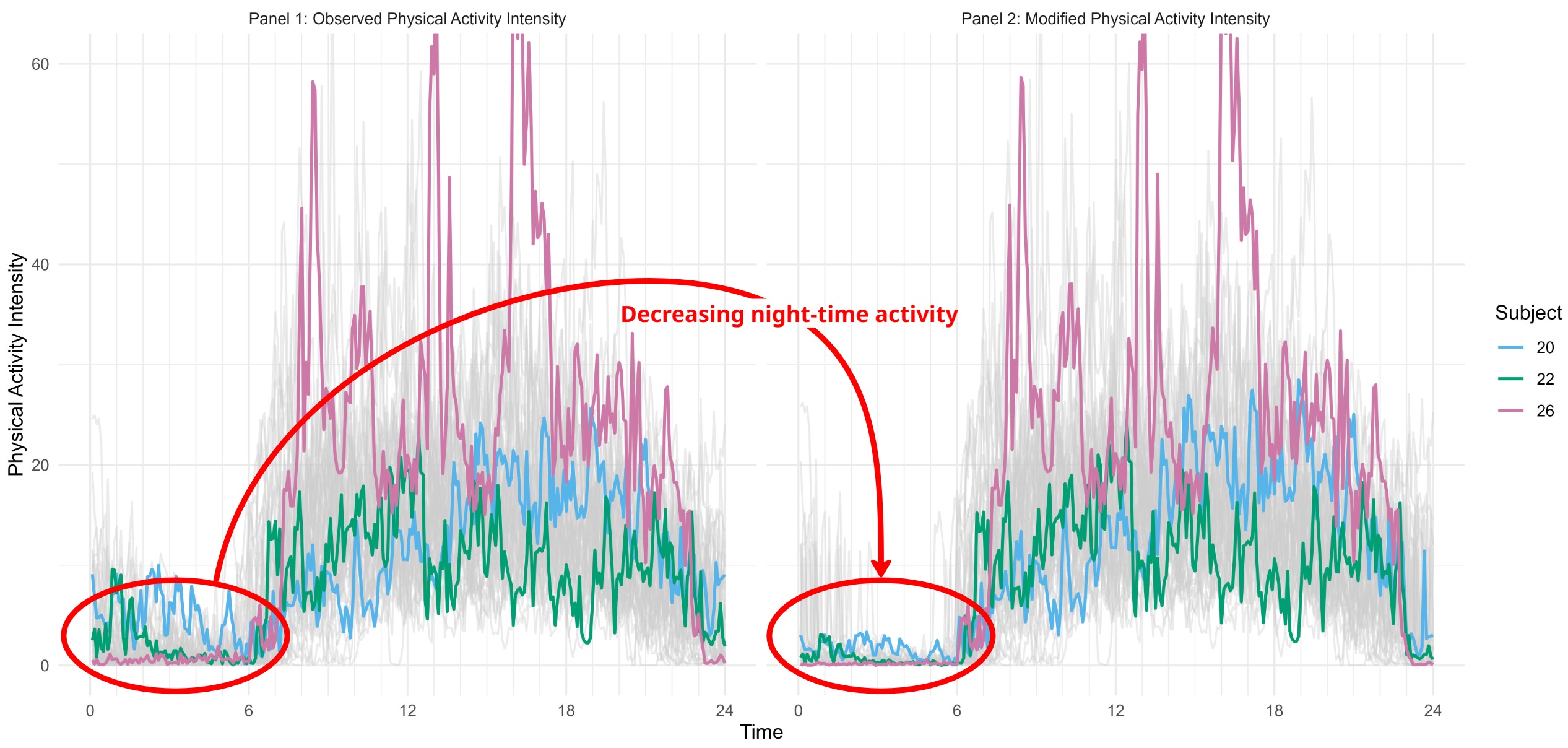
Many real-world interventions for causal inference are inherently multi-dimensional or continuous — ventilator pressure–time curves, daily physical activity trajectories, multi-component drug regimens, and dose–duration combinations. My research develops a unified framework of modified treatment policies for such settings, covering continuous-valued, vector-valued, and functional treatments. Within this framework I target data applications where the treatment cannot be reduced to a simple binary contrast. In critical care, I use the multivariate modified treatment policy (MVTP) to estimate the causal effect of mechanical ventilation on ventilator-induced lung injury, treating the joint settings of tidal volume, positive end-expiratory pressure, and driving pressure as a vector-valued exposure. In wearable-sensor studies, I use the modified functional treatment policy (MFTP) to estimate causal effects of entire daily physical activity trajectories, where each subject’s treatment is a curve rather than a single summary statistic.
Multiway & Functional Data analysis
Modern biomedical data are often high-dimensional (e.g., spanning multiple cell types, tissues, or body regions) or measured over a continuum (e.g., continuous activity curves from wearable devices). I develop Bayesian methods for analyzing such data, including BAMITA, a Bayesian multiple-imputation method for tensor (multiway) data; BAMIFun, a Bayesian multiple-imputation method for functional data; and a Stan-based tutorial and software package (refundBayes) that makes Bayesian functional regression — with scalar, functional, or survival outcomes and flexible functional predictors — broadly accessible to applied researchers.
Evidence Synthesis & Causal Generalizability
Regulatory and health-technology decisions almost never rest on a single trial; they must synthesize heterogeneous evidence — different populations, different comparators, aggregate vs. individual-patient data. My work develops and evaluates methods that transport causal effects across study populations in this setting. I have contributed a comprehensive review of matching-adjusted indirect comparison (MAIC) and a companion R Shiny tool, a critical assessment of MAIC under violations of common assumptions, and methodology for combining hazard ratios in indirect treatment comparisons. I also develop meta-analytic methods for reference-interval estimation from individual-patient data (and an accompanying R Shiny app, RIMeta), and hierarchical models for heterogeneous readmission prediction across hospitals.
Innovative Clinical Trial Design
Modern trials — platform trials evaluating many arms over time, basket trials studying one therapy across multiple indications — can sharply reduce cost and time to evidence, but introduce non-trivial statistical challenges: treatment arms enter and leave at different calendar times, the shared control accrues across periods, and indications differ in prognosis. I work on statistical strategies that leverage this structure responsibly, including methods for borrowing from nonconcurrent controls while preserving Type I error, adaptive borrowing from concurrent controls across periods, and the use of external control arms (real-world or historical) to augment small basket-trial indications. The goal is efficiency gains that a regulator can audit.